
Lesson 1- Orientation: What Are We Even Looking At
One of the biggest misconceptions about dissociation is that it’s rare and easy to identify.
Many people imagine dissociation as something dramatic or obvious. They picture severe memory loss, distinct identities, or experiences that are immediately recognizable. While those presentations certainly exist, they represent only a small part of the picture.
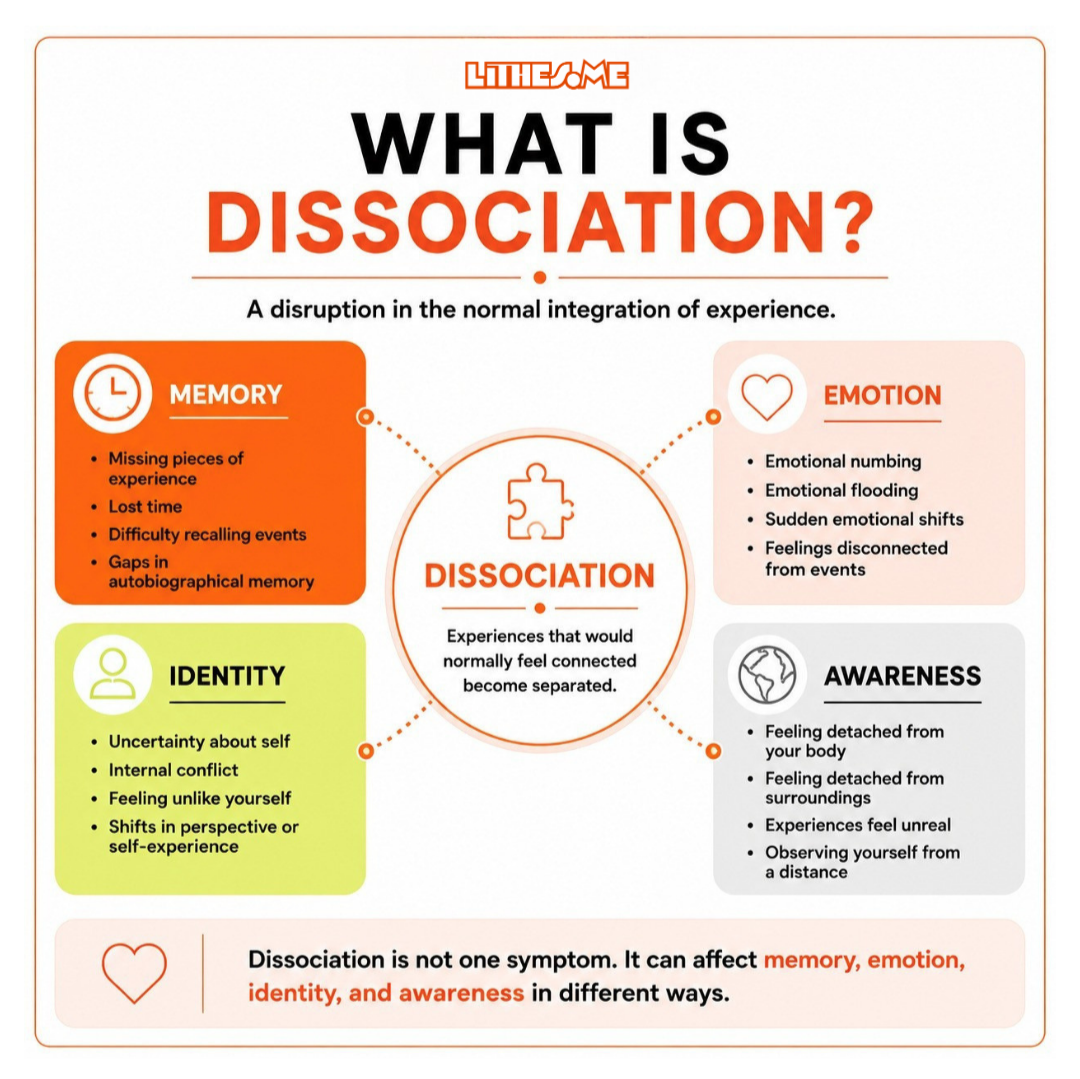
Before we explore how dissociation presents in clinical practice, it’s helpful to begin with a simple understanding of what dissociation actually is. At its broadest, dissociation refers to disruptions in the integration of psychological experience. Experiences that are typically connected, such as thoughts, emotions, memories, body sensations, identity, or awareness, may become experienced as less connected or more compartmentalized.
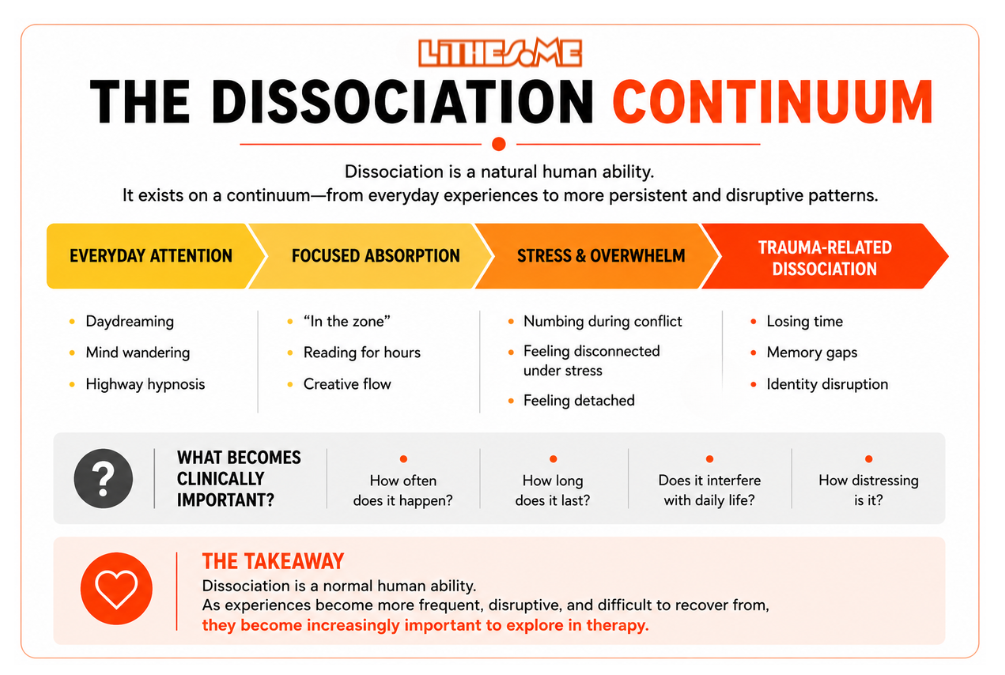
One of the most important things to understand is that dissociation exists on a continuum.
Mild dissociative experiences are a normal part of being human. Most of us have experienced becoming completely absorbed in a book, arriving home and realizing we don’t remember part of the drive, daydreaming during a lecture, or becoming so focused on a task that we lose track of time. These experiences reflect our mind’s natural ability to shift and narrow attention.
As experiences become more frequent, more disruptive, or begin interfering with daily life, they become more clinically relevant. This doesn’t automatically mean someone has a dissociative disorder, but it does invite us to become more curious about what’s happening.
Most clients aren’t going to walk into therapy and say, “I think I’m dissociating.” More often, they describe experiences that feel confusing, disconnected, inconsistent, blurry, or difficult to explain.
They may say things like:
- “I zone out sometimes.”
- “I don’t feel fully here.”
- “I lose track of conversations.”
- “Parts of my life feel blurry.”
- “I feel disconnected from myself.”
- “I don’t know why I reacted like that.”
- “Sometimes I don’t feel real.”
- “I feel numb.”
At first glance, these experiences can easily get sorted into more familiar categories like anxiety, depression, ADHD, overwhelm, burnout, panic, or emotional dysregulation. Sometimes those explanations fit. Other times, they only explain part of what the client is experiencing.
This course isn’t about immediately diagnosing dissociative disorders. It’s about learning to notice when something in the clinical picture feels disconnected, inconsistent, difficult to track, or only partially explained by the symptoms on the surface.
Many therapists receive little formal training in dissociation during graduate school. As a result, many clinicians enter the field assuming it’s something they will rarely encounter unless they specialize in trauma or severe psychopathology. In reality, dissociation appears across many different clinical presentations and often hides beneath symptoms that are easier to recognize. That is one of the reasons it is so frequently overlooked.
Clients may spend years in therapy talking about anxiety, depression, panic attacks, emotional numbness, relationship instability, substance use, eating disorders, or feeling chronically “stuck,” while the underlying disconnection is never directly explored.
The goal of this lesson isn't to make you hypervigilant for dissociation or assume it's everywhere, it's to begin building awareness around experiences that do not fully connect or make sense through the lens of symptoms alone.
At this stage, you're learning how to slow down and notice. You're learning to pay attention to:
- Moments of disconnection
- Vague or difficult-to-describe experiences
- Inconsistencies in memory or emotional experience
- Shifts that feel confusing to the client themselves
- Symptoms that do not fully explain the whole picture
You're beginning to develop a different kind of clinical observation.
Short Clinical Vignette
A client says:
“I think I’m just stressed out. Sometimes I drive home and barely remember the drive. I’ll be talking to someone and suddenly realize I stopped listening halfway through. At work I kind of zone out sometimes and then panic because I missed something important.”
The client doesn't identify this as dissociation. They describe it as stress, exhaustion, anxiety, or burnout.
At this stage, you don't need to immediately label the experience. Instead, stay curious and begin noticing the pattern.